The seismocardiogram as magnetic-field-compatible alternative to the electrocardiogram for cardiac stress monitoring
Executive Summary
This study demonstrates the feasibility of using seismocardiography (SCG) as a magnetic-field-compatible alternative to electrocardiography (ECG) for monitoring cardiac function during MRI stress testing. SCG waveforms were shown to remain unaffected by flow-induced electrical artifacts that distort ECG recordings in MRI environments. Experiments in a porcine model revealed that changes in SCG amplitude at aortic valve opening correlate with left ventricular function assessed via cine MRI, providing a sensitive indicator of myocardial ischemia onset.
Answer Machine Insights
Q: How does SCG compare to ECG in detecting ischemia during MRI?
SCG is unaffected by flow-induced electrical artifacts that distort ECG recordings in MRI environments, making it a more reliable tool for ischemia detection.
The superposition of voltages induced by blood flow in a strong magnetic field generally prevents the detection of changes on the ECG, such as ST segment changes, that are indicative of myocardial ischemia. SCG may represent a useful, MRI-compatible alternative to the ECG for monitoring patients subjected to pharmacological stress during an MRI examination.
Q: What physiological changes were observed in the porcine model during LAD stenosis?
SCG amplitude at aortic valve opening decreased significantly, correlating with reduced ejection fraction and impaired myocardial wall thickening.
The ejection fraction, calculated from cine MR images, decreased from 74% at baseline, to 32% during severe stenosis. The myocardial perfusion measurement with radio-isotope labeled microspheres indicated that blood flow in the territory of the LAD decreased from 1.1 ml/min/g at baseline, to 0.3 ml/min/g during severe stenosis.
Key Results
SCG amplitude at aortic valve opening decreased significantly during severe LAD stenosis, correlating with reduced ejection fraction (74% to 32%).
SCG waveforms remained unaffected by MRI-induced electrical artifacts, unlike ECG recordings.
Visual Evidence
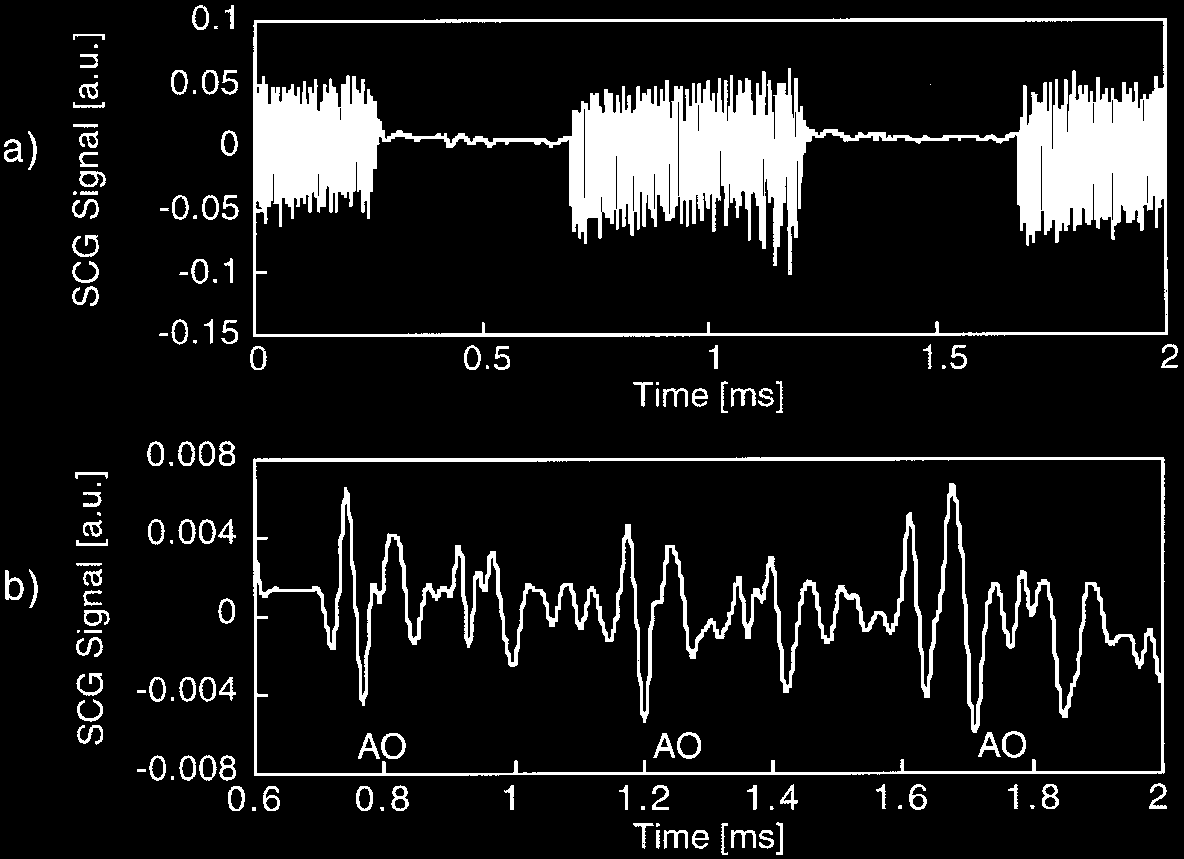
Figure 3. SCG traces recorded in a normal volunteer while the magnetic ®eld gradients are being pulsed for acquisition of cine MRI images. A low pass Butterworth ®lter with a cut-o frequency of 30 Hz was applied to the trace shown in part (a), and the result is shown in (b). The amplitudes at aortic valve opening labeled with AO in (b) are clearly recognizable on the ®ltered waveforms.
Clinical Snapshot
Evidence Rating
Relevance
high Priority