Evaluation of seismocardiography in detecting pre-load changes and cardiovascular disease: a comparative study with transthoracic echocardiography
Executive Summary
This study evaluates the ability of seismocardiography (SCG) to detect pre-load changes and differentiate cardiovascular disease (CVD) conditions, comparing its performance with transthoracic echocardiography (TTE). Using a cohort of 26 subjects, SCG demonstrated sensitivity to pre-load alterations induced by isotonic saline infusion, with significant changes in diastolic amplitudes and time intervals. While SCG did not distinguish between healthy and CVD groups, it identified differences in diastolic amplitudes between infusion-tolerant and infusion-intolerant subjects, suggesting potential utility in detecting diastolic dysfunction and left ventricular filling pressures.
Answer Machine Insights
Q: Can SCG detect pre-load changes in subjects with cardiovascular disease?
Yes, SCG detected significant changes in pre-load conditions induced by fluid infusion, including alterations in diastolic amplitudes and time intervals.
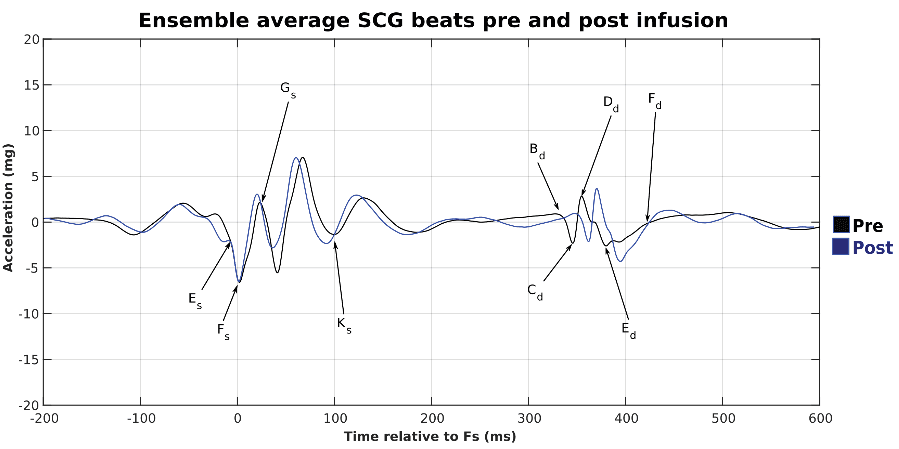
SCG showed significant differences before and after changes in pre-load induced by infusion of isotonic saline. SCG were able to detect significant differences in amplitudes Dd, Ed, and Ls and most of the time intervals.
Q: Does SCG differentiate between healthy individuals and those with cardiovascular disease?
No, SCG did not detect significant differences between healthy and CVD groups in this study.
No significant difference was observed when comparing the healthy and CVD groups in both pre- and post-infusion.
Key Results
SCG detected significant changes in diastolic amplitudes (e.g., Dd increased by 23%, P = 0.016; Ed decreased by 48%, P < 0.001) and time intervals after fluid infusion.
SCG diastolic amplitude Cd-Dd showed significant differences between infusion-tolerant and infusion-intolerant groups (pre-infusion: 7.7 vs. 3.7 mg, P = 0.046; post-infusion: 8.3 vs. 4.1 mg, P = 0.034).
Visual Evidence
Clinical Snapshot
Evidence Rating
Relevance
high Priority