Accurate Detection of Dobutamine-induced Haemodynamic Changes by Kino-Cardiography: A Randomised Double-Blind Placebo-Controlled Validation Study
Executive Summary
This study introduces and validates Kino-Cardiography (KCG), a novel non-invasive technique combining ballistocardiography (BCG) and seismocardiography (SCG) to measure 12 degrees-of-freedom (DOF) body motion. Using a randomized, double-blind, placebo-controlled crossover study with 34 healthy subjects, KCG demonstrated high accuracy (96.9%) in detecting dobutamine-induced hemodynamic changes. KCG metrics, including kinetic energy (iK) and power (Pmax), correlated strongly with echocardiographic measures of stroke volume (r = 0.71) and cardiac output (r = 0.8), suggesting its potential for monitoring cardiac contractility in clinical practice.
Answer Machine Insights
Q: How accurate is KCG in detecting dobutamine-induced changes?
KCG demonstrated an accuracy of 96.9% in distinguishing dobutamine infusion from placebo.
KCG sorted dobutamine infusion vs. placebo with 96.9% accuracy.
Q: What is the correlation between KCG metrics and echocardiographic measures?
KCG metrics showed strong correlations with stroke volume (r = 0.71) and cardiac output (r = 0.8).
Increases in SV and CO were correlated to iK (r = +0.71 and r = +0.8, respectively, p < 0.0001).
Key Results
KCG sorted dobutamine infusion vs. placebo with 96.9% accuracy.
Correlation coefficients: Stroke Volume (r = 0.71), Cardiac Output (r = 0.8).
Visual Evidence
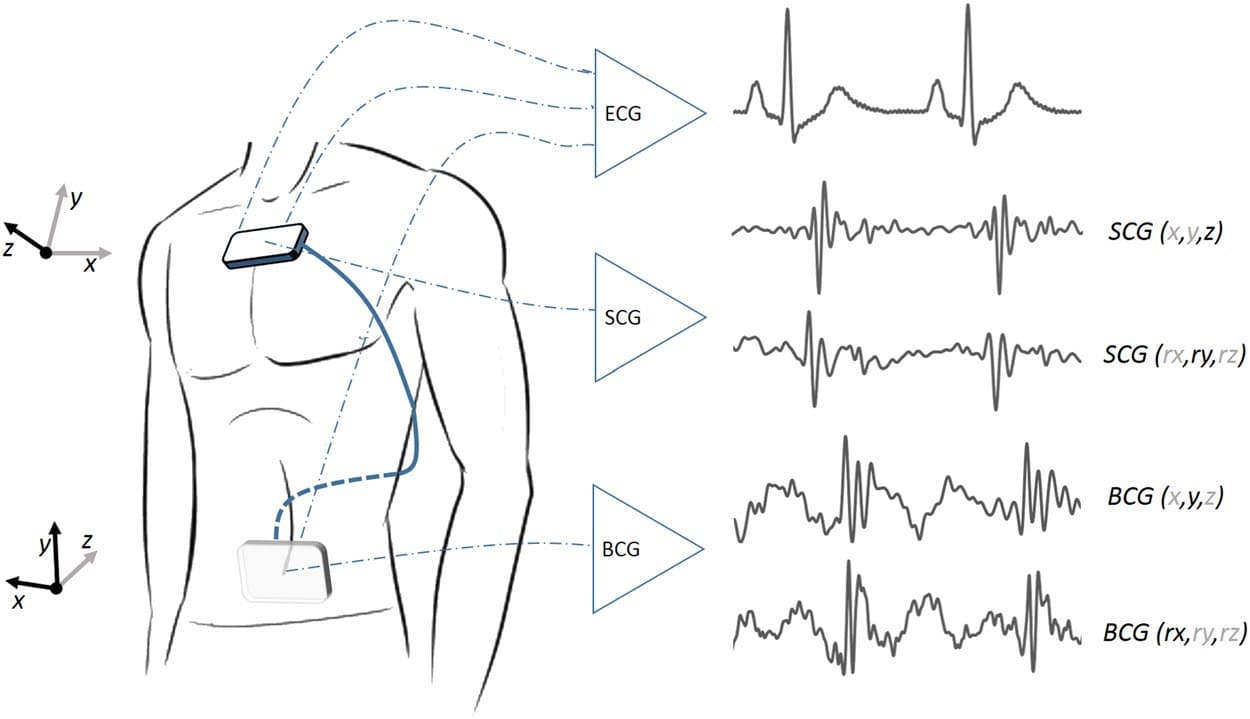
Figure 2. Kino-cardiograph device measuring 2-lead ECG, 6-DOF seismocardiography (SCG) and 6-DOF ballistocardiography (BCG). The standard axis system is used for BCG and SCG: BCG x, y, and z are respectively left-to-right, caudocranial, and ventrodorsal axes; SGC x, y, and z are respectively right-to-left, caudocranial, and dorsoventral axes.
Clinical Snapshot
Evidence Rating
Relevance
high Priority