Influence of sympathetic activation on myocardial contractility measured with ballistocardiography and seismocardiography during sustained end-expiratory apnea
Executive Summary
This study investigates the relationship between sympathetic activation and myocardial contractility using ballistocardiography (BCG) and seismocardiography (SCG) during sustained end-expiratory apnea. The researchers measured kinetic energy (iK) from BCG and SCG signals alongside muscle sympathetic nerve activity (MSNA) using microneurography in healthy male participants. Findings reveal that linear iK from BCG correlates strongly with sympathetic activity, particularly at the end of apnea, suggesting its potential for assessing autonomic changes in sleep-related disorders.
Answer Machine Insights
Q: How does BCG compare to SCG in assessing sympathetic activity during apnea?
BCG shows stronger correlations with sympathetic activity, particularly in the linear dimension, compared to SCG.
Linear iK of BCG is directly and more strongly related to the rise in sympathetic activity than the SCG, mainly at the end of a sustained apnea.
Q: What physiological changes occur during sustained apnea?
Sympathetic nerve activity increases, oxygen saturation decreases, and cardiac kinetic energy rises, particularly in the linear dimension of BCG.
At the end of the apnea compared with normal breathing, changes in iK computed from BCG were related to changes of tMSNA and BF only in the linear dimension.
Key Results
Linear iK from BCG increased by 58% during the second third of apnea compared to baseline (P = 0.02).
Strong correlation observed between changes in linear iK of BCG and total MSNA at the end of apnea (r = 0.85, P < 0.0001).
Visual Evidence
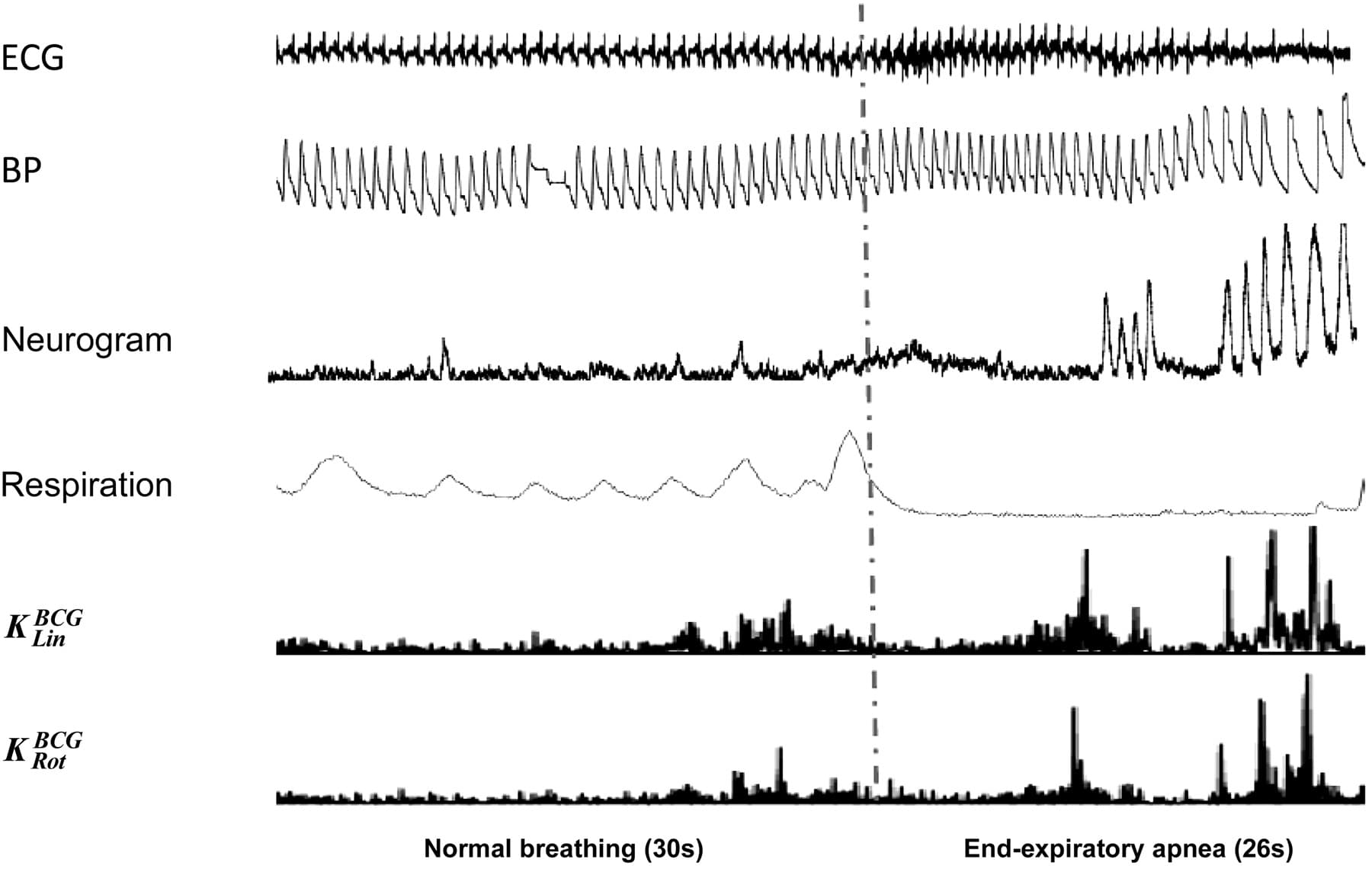
Fig. 2. Muscular sympathetic nerve activity (MSNA) variations along with linear kinetic energy (KLin) and rotational kinetic energy (KRot) of ballistocardiography (BCG) during baseline and maximal end-expiratory voluntary apnea. Normal respiration (30 s long) and maximal voluntary end-expiratory apnea (26 s long) are sep- arated by the vertical dotted/dashed gray line. From top to bottom: ECG, blood pressure (BP), neurogram, respiration, KLin of BCG, and KRot of BCG. At the begin- ning of the apnea, there is a suppression of the sympathetic nerve activity without discernable bursts along with mild cardiac kinetic energy recorded with the BCG in both the linear and the rotational dimension. Heart rate (HR) accelerates compared with normal respiration, and systolic BP slightly falls. Toward the end of the apnea, a marked rise in the sympathetic nerve activity is observed, characterized by an increase in BF and total MSNA (tMSNA), and this is accompanied by a marked increase in linear and rotational kinetic energy. HR slows and systolic BP rises compared with the beginning of the apnea. BF, burst frequency (burst/min).
Clinical Snapshot
Evidence Rating
Relevance
high Priority