Non-Invasive Wearable Patch Utilizing Seismocardiography for Peri-Operative Use in Surgical Patients
Executive Summary
This study introduces a wearable patch that combines seismocardiography (SCG) and electrocardiography (ECG) signals to estimate stroke volume (SV) in peri-operative surgical patients. Using a random forest regression model validated with leave-one-subject-out cross-validation, the wearable patch achieved a correlation coefficient of 0.81 and a median absolute error of 7.56 mL compared to the Transesophageal Doppler (TED) reference standard. The findings suggest that this non-invasive technology could replace TED for continuous SV monitoring during pre-, intra-, and post-operative periods, improving fluid management protocols and patient outcomes.
Answer Machine Insights
Q: How accurate is the wearable patch compared to the TED for stroke volume estimation?
The wearable patch achieved a correlation coefficient of 0.81 and a median absolute error of 7.56 mL compared to the TED.
The regression model trained on the combination of the SCG and ECG features was correlated to the TED reference standard (r = 0.81) with a relatively low MedAE (7.56 mL) across all subjects.
Q: What are the advantages of using SCG and ECG signals together for stroke volume estimation?
Combining SCG and ECG signals improves prediction accuracy, achieving higher correlation and lower error compared to using either signal alone.
Using the cardio-mechanical information only (i.e., SCG signal features alone) resulted in a correlation value of 0.67 and a MedAE of 9.51 mL, whereas using only the electrical (ECG) information resulted in a correlation value of 0.31 and a MedAE of 14.75 mL.
Key Results
Correlation coefficient of 0.81 between wearable patch predictions and TED reference values.
Median absolute error of 7.56 mL for stroke volume estimation using SCG and ECG features.
Visual Evidence
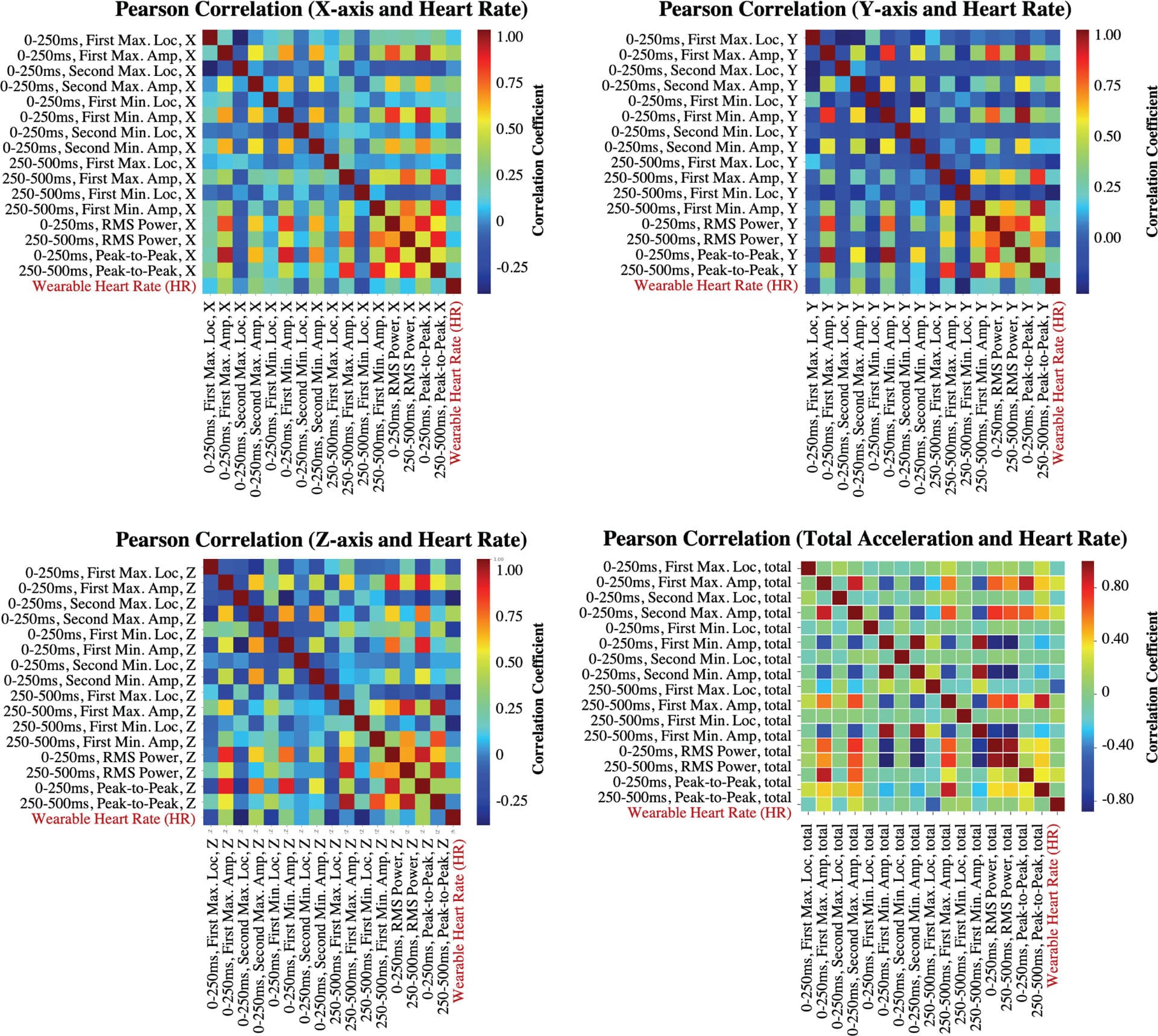
Fig. 6. Pearson correlation coefficients between different feature pairs from SCGx,y,z,total signals.
Clinical Snapshot
Evidence Rating
Relevance
high Priority